


















Striate arteries or Ganglionic arteries arise from the middle cerebral artery and supply deep structures in the cerebrum including the internal capsule and reticular formation. Strokes in these vessels are common and can cause extensive damage. This is because emboli are carried up the carotid and tend to be swept into the MCA, sometimes called the artery of stroke, and are prone to getting stuck at this branch point in the Sylvian fissure.
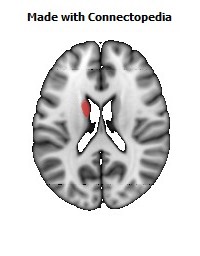
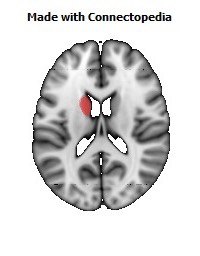
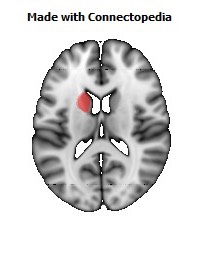
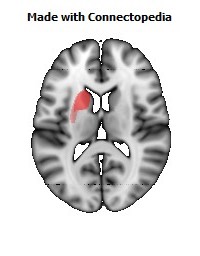
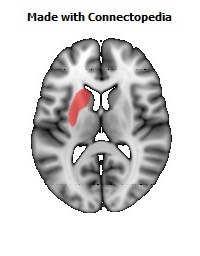
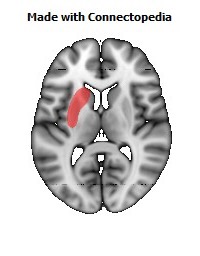
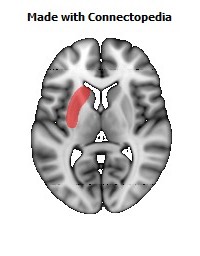
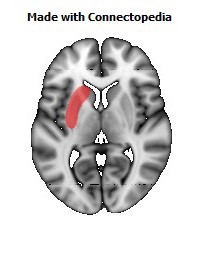
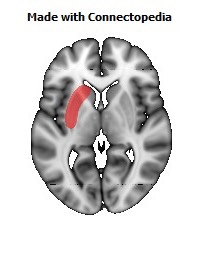
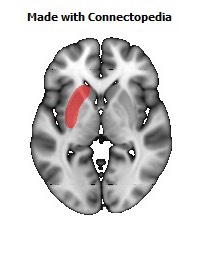
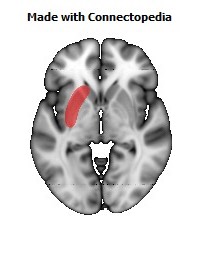
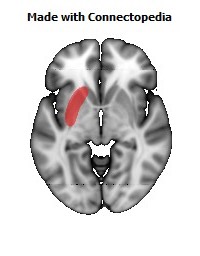
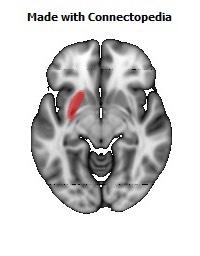
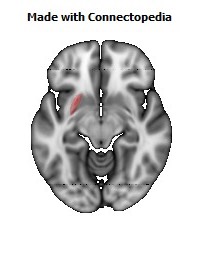
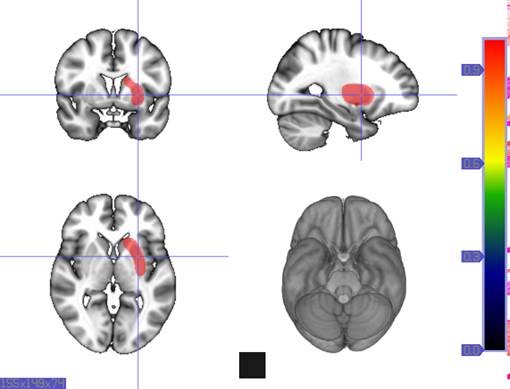
The middle cerebral artery (MCA) is a large diameter vessel that branches at an acute angle from the internal carotid artery. The MCA passes laterally just underneath the frontal lobe, ultimately taking up a position between the temporal and frontal lobes in the Sylvian fissure. The initial part of the MCA is a single vessel called the stem or M1 segment. As it passes laterally, the stem gives off a series of six to twelve long, small diameter, penetrating vessels that travel directly upward to supply the basal ganglia and much of the internal capsule. These are called the lenticulostriate arteries. These small arteries are particularly susceptible to damage from hypertension. They may either rupture, producing an intracerebral hemorrhage that is initially centered in the region they supply, or become occluded producing a lacunar infarct in the tissue they supply. The lenticulostriate arteries are 'end arteries' meaning that the regions they supply do not have significant collateral blood supply. Occlusion of these vessels therefore leads to stereotyped stroke syndromes.
In the case of the lenticulostriate vessels, hemorrhage may remain localized to the putamen and caudate nucleus, may involve neighboring structures like the internal capsule and other more distant white matter of the hemisphere, or may even rupture into the ventricular system. Lacunar infarcts may have serious functional consequences if they involve motor or sensory fibers in the internal capsule, but may be 'silent' if they involve other small regions of white matter or the basal ganglia.